
Nasal Polyposis In Cystic Fiborsis



Cystic fibrosis should be suspected in any child which fails to thrive with malabsorption or rectal prolapse; with chronic or recurrent cough with sputum; or with cirrhosis portal hypertension. Difficulties arise where there is little involvement of either the pancreas or lung or when manifestations appear in older children or even later. Evidence should be sought for pancreatic insufficiency. The high concentration of sodium in sweat parotid secretion is of major diagnostic value. The normal sweat sodium concentration rises from a mean value of 22 mmoi/i in infancy to 55 mmoi/i in adults. Values above 70 mmoi/i are diagnostic in infants, but not so in adolescents adults. In cystic fibrosis, however, the fall in sweat sodium concentration after 9a - fluorohydrocortisone is usually less than 10% whereas in normals the fall is much greater. With respiratory infection there is usually a polymorphonuclear leucocytosis. The chest radiograph may show only parallel line shadows cast by bronchial walls in the more peripheral parts of the lung. Ill - defined nodules or patchy clouding up to 10 - 20 mm in size may appear these shadows may cavitate. Ring shadows honeycombing, segmental or lobar consolidation with or without atelectasis usually under 1 - 2 years of age, enlarged hilar nodes are also seen. None of these shadows are diagnostic alone, but in the aggregate they are very characteristic.
Etiology: - chronic naso - pharyngeal allergy. Chronic bacterial viral infection. Vasomotor disturbances.
Symptoms: - *onset insidious. * nasal obstruction, uniateral or bilateral.*anosmia, *epiphora.* post nasal drip.* snoring.
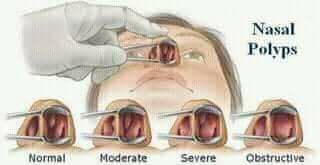
Signs:- reveals ethmoidal polypi. Bilateral. Multiple other.
Patient homeopathic treatment for symptomatic signs or other sig base medician apply.



+1.svg)
